
- Home
- About author
- About discovery
- Publications
- Cases from practice
- What do we treat
- To patients
- Partnership
- Comments
- FAQ
- Site map
- Demodecosis
- Acariasis
- Etiology
- Pathogenesis
- Clinic
- Diagnostics
- Treatment
- Prevention of acariasis
- Prevention of any diseases
- House dust mites
- Common with allergy
- Difference from allergy
- Allergy
- Etiology
- Pathogenesis
- Clinic
- Diagnostics
- Allergy diseases
- Treatment
- Prevention of allergy
- Prevention of allergic shock
- Prevention of any disease
- Common with acariasis
- Difference from acariasis
- Documents
ABOUT THE PRESENCE OF PANDEMIC ACARIASES ON THE PLANET
Autor:
Rakhima D. Zhaxylykova, Aisulu D. Ahimova
At present the scientific literature and the periodical press are full of the information testifying the mites activation. According to our repeatedly checked data of scientific researches, which were conducted for more than 35 years, demodexes, dermatophagoideses and other mites, which have become constant residents of our environment, cause the homonymous acariasis, which acquired the pandemic dissemination. Acariasis is progressing because of the lack of the dedicated control. The most serious manifestations and complications of acariasis are registered in medicine under the mask of known allergenic, skin, rheumatic, cardiovascular, oncological and other diseases. The most important for diagnostics, medical treatment and prophylaxis of demodectic, dermatophagoidic and other acariases is the best knowledge of its clinics. For liquidation of acariases it is necessary to consolidate the efforts of medical employees, acarologists, engineers, pharmacists, employees of social and government spheres and others.
INTRODUCTION
The clinical medical acarology is the less developed field. Some aspects of clinical acarology are covered by the specialists from different fields: infection disease doctors, dermatologists, epidemiologists, rheumatologists, allergists, acarologists, veterinarians, microbiologists and others.
Among the variety of acaries, the ticks (Ixodidae, Argasidae and part of Gamasidae) are known as carriers of different human infection diseases. Their stings invoke typical disease representation in human’s skin and hypoderm. Moreover, acaries open the entry to the skin for other microorganisms (Cunha, 2001; Zhaxylykova, 2007d). Mites (they are more in species and quantity) beside the described above are able to cause diseases united under the general title of scab (synonyms: acariasis, acarosis, mite’s dermatitis and others). Detrimental action of acaries expresses in the capacity of any representations to suck on the human at presence of specified conditions (for example, lack of other food) (Walter and Proctor, 1999; Zhaxylykova, 2007e).
During more than eighteen centuries the different manifestations and complications of classical scab, caused by Sarcoptes scabiei, from the skin and internals had been raging among people. For a long time the main cause of development of these diseases was considered as incorrect fluid mixture of human organism. Even after indisputable proof of invasive disease nature - separation from pathologic skin elements of acary Sarcoptes scabiei and its viewing under microscope, there were scientists, who thought that the scab is non-contagious disease. Now it is recognized that the classical scab is infectious disease and is caused by Sarcoptes scabiei (Sokolova, 2001;Zhaxylykova, 2007f).
In the middle of XIX century on the skin of sick people with the classical scab researchers found demodexes (since 1841-1843) and dermatophagoideses (since 1863). At present in different corners of the planet the careful research of the skin of a sick with classical scab the scientists quite often find both demodexes and dermatophagoideses. However, these findings do not receive due attention. No one attempts to remove the found in the skin mites. At the same time scabiologists and dermatologists ascertain that people who had a classical scab often feel itch and dryness of the skin. Experts consider that this condition is the residual phenomenon after the tolerated classical scab and name it postscabies itch or acarophobia (Ponomarev et al., 2000; Zhaxylykova, 1992b).
In 1841 the demodexes were found in 100% of examinations of the skin of people with ill and with "healthy" skin. Attempts to clear the skin from demodexes of some dermatological patients with antiparasitic treatment were not a success. Therefore, in the 50-s of XIX century demodexes have been ranked as saprophyte microorganisms of the human skin. Meanwhile the medical literature mentions that even before Christ demodexes were considered the activators of almost all skin diseases of people. For animals Demodex unambiguously are considered as parasites. Demodecosis (demodectic acariasis) for animals is studied and described, and better of all - for dogs. Researchers note that in the neglected cases demodecosis of dogs causes fetid smell, result in their exhaustion (cachexy), and perish. At detection demodexes in the skin of animals on the herd is put on quarantine, the sick animal is isolated and serving personnel is required to strictly observe the certain sanitary regime. The corpse of the fallen from demodecosis animals burn or dig in the ground on depth not less than two meters (Baker, 1999, Vasilevich and Larionov, 2001). It is a paradox but the fact: for people Demodex is considered as saprophytes, which only at presence of aggravating circumstances (infringement of function of the gastroenteric path, development of endocrinology shifts in the organism, after strong stresses, etc.) is capable to lead to development of disease. Today the recognized opinion in medicine about Demodex is that it is the activator of discoid red lupus, red acne and demodectic blepharo-conjunctivitis. At the same time in the scientific literature there is a message about heavy system affection of an organism of a person with demodecosis under the name of «demodecosis-gravis». It is necessary to emphasize that demodecosis in medicine was never purposefully studied, and described in the literature works were performed by some scientists-enthusiasts (Zhaxylykova, 1990).
The discoverers considered feather mites (dermatophagoideses) the activators of a special version of scab, which was named by them dermascab. In their opinion, dermascab itch is characterized by persistent, untreatable skin itch. The authors write that dermatophagoideses live deeply in the skin of the person and eat his blood. However, in the literature on clinical medicine we did not find the cases of the description of diagnostics and treatment of this version of a scab. At the same time, researchers everywhere note the abundance of dermatophagoideses on the skin of the pilary part of the head most often at people with the high level of hygiene.
After discovery of dermatophagoideses acarologists in different corners of the planet discover and describe other kinds of mites. This process continues to this day.
During XX century researchers with surprise ascertain the fact of detection of various mites in the dust of any places of stay of people, and their quantity and number of species is growing. Almost in all the countries of the world in the household and industrial dust the mites of Dermatophagoides kind prevailed. In the 60-s of the last century the Dutch scientists (Voorhorst et al.) represent an incontestable fact of participation of dermatophagoideses in occurrence and development of respiratory allergosis and so-called atopic variants of the bronchial asthma of people. Researchers note that the disease arise as a result of sensitization of the organism of the person to components of the remains of bodies and excreta of mites. The numerous facts described in the scientific literature of detection of mites in excreta, organs and fabrics of people (even in thickness of the atherosclerotic lamina of aortas of a human) are interpreted as casual. No attention is paid to the described cases or even to small epidemics pulmonary acarosis, gooseberries illnesses, mites dermatites, mites gastroenterocolitis and others (Agadzhanjan and Savelyeva, 1997; Bogdanova, 2005).
Quite often in the literature on dermatology and scabiology it is possible to meet the following paradoxical fact. Some people having no typical signs of classical scab have scabby mites Sarcoptes scabiei in their skin. Experts consider such condition a healthy carriage of scabby mite by a human. This condition even has the scientific name - acarotregerstvo.
Almost all the researchers who study demodexes and other mites ascertain that on the surface and inside of the bodies the mites carry more smaller microorganisms: bacteriums, viruses, fungis, eggs of helminthes and others (Semenov et al., 2002).
Now both the scientific literature and periodical press are full of information testifying activation of acaries. Ticks inhabit our parks, courtyards, houses and sometimes - apartments. As to small relatives of acaries, over 200 their kinds became almost constant inhabitants of residential houses, industrial, subsidiary premises and any other places of stay of people. Besides, some kinds for many decades live in bed of a human, his underwear and even in the skin (Gerson et al., 2003; Kiseleva, 2007; Surovenko and Zheleznova, 2002).
It is believed that demodexes eat cast-off epithelium and contents of glandula of the skin. The food of dermatophagoideses considered to be the cast off in bedding epithelium of the human skin. It is necessary to note that a similar opinion, which appeared to be erroneous, existed in medicine about lice. For a long time it was believed that lice eat the cornified epithelium of human skin. Actually they bite the person and eat his blood. Or another example: the official medical science for long time did not recognize existence of viruses. The first virologists were laughed at, declaring, that they have a hole either in filters or in the head. And now the virology has taken a worthy place in medicine.
At present the situation in the medicine in relation to the demodexes and dermatophagoideses reminds the story with the sarcoptic scab. Though demodexes are found in 100% in the skin and dermatophagoideses in the skin, excreta and close environment of the people, the first are reckoned among the saprophytes causing illnesses in exceptional cases, while for the second only their excreta and remains are considered to be mechanical and allergic irritants. Presence of objective changes on the skin of carriers of these mites experts explain to be the result of manifestations of various diseases of internal organs (gastrointestinal tract, endocrine glands, impact of stress, etc.).
The statistics of sickness rate of people in medicine is now depressing. Despite of sufficient development of the medical science and high development of medical technique, quantity of illnesses of people continues to grow (Belousova, 2003; Gromnatskij 2005). Excessively narrow specialization has led now to the fact that the number of medical specialties already exceeds the quantity of organs of the human body. But the world is uniform and continually reminds about this to people. According to Veterinary Committee of the World Health Organization (WHO) there are more than 150 diseases common for a human being and animals. For example, there are described cases of a mange transition (animals have several versions of it) from house and wild animals to people and vice versa. From these facts a conclusion can be drawn about necessity to control not only people’s own health, but also health of animals.
Catamnesic studying of disease of people shows growth of cardiovascular, gastroenterological, skin, allergic, endocrinological, neurological, oncological and other illnesses quantity. Also the number of people with the whole bouquet of the most different illnesses has increased. The basic problem of public health services in the majority of economically developed countries are so-called chronic noninfection diseases (NID), among which there are allergic, skin, rheumatic, oncologic, etc. In the 70th years of the expired century the scientists who have studied NID epidemiology distributions, ascertained that these illnesses have infectious character of distribution. Now allergists and dermatologists firmly declare that allergic and skin illnesses extend epidemically. Besides, the number of infectious diseases, from which the person of XXI century suffers, also increases (Lobzin et al., 2000). Now the WHO ascertains that health of the modern person by 40% depends on the environment and heredity, by 10% - from medicine and by 50% -on conditions and way of life.
Allergists and immunologists established that components of bodies and excreta of any acaries are alien, that is allergenic for a human body. It is an axiom. Antibodies are always formed for allergens in immunocompetent organism. It is an axiom too. Presence of antibodies in blood of sick people on components of bodies of demodexes, dermatophagoideses and sarcoptids are found out by many researchers, such as Vartapetov, Vaisblatt, Voorhorst, Jagofarov, and others. Besides scientists mark that structural components of parasites bodies for a long time living in the macroorganism gradually change to similar or close to components of their owners (Lobzin et al., 2000).
MATERIALS AND METHODS
Being the gastroenterologist-researcher, 35 years ago we have met a casual fact: on the patient, who was hospitalized with a chronic hepatites at the stage of aggravation, from pathologically changed part of the face skin (the diagnosis «Discoid red lupus») dermatologists-advisers found a great amount of Demodex folliculorum. Paradoxical for us then was the statement of experts that this patient is not dangerous for surrounding people. Therefore we have started to carefully observe the skin condition of all the people surrounding this patient: neighbor in the chamber, other patients who contacted with her, serving medical personnel, visitors of the chamber, etc. Within the next six years we had three patients with the similar pathology of the face skin. The described above supervision we carried out for all people surrounding these patients, including children. We fixed the revealed changes in dynamic either in the history of illness or in a notebook. We revealed a regularity, which contradicted statements of dermatologists-advisers: demodecosis was transferred to surrounding people with healthy skin quickly enough at the direct and mediated contact, progressed in due course. Automatically we were switching to supervision over the condition of the skin of the open parts of the body of all people surrounding us where we were. There was a period when these supervisions allowed us to receive the information on a degree of close contact (ridiculously!) colleagues and friends among themselves by character of the arisen affection of the skin by mites (not without reason now the scab is considered to be a disease transferred by sexual contacts. Demodecosis is a version of scab). During supervision demodecosis quickly enough spread among people with healthy skin (Zhaxylykova, 1991).
Among patients and people surrounding us there were many of those who already had affected by demodexes skin. To be sure of the degree of influence of demodexes on clinical course of the basic disease and an objective condition of the integument we have entered some corrective amendments into treatment of the patients. One patient received the treatment planned on the basic scientific subjects. In parallel other patients besides such treatment received external antiparasitic treatment. As a result there were 268 people, of them 137 patients received external antiparasitic treatment and 131 persons did not.
In order to define specific weight of persons with the skin affected by mites in various branches of the Republican Clinical Hospital (RCH), gastroenterological branch in which was based our clinical department of dietetic therapy of the Scientific Research Institute (SRI) of the Regional Pathology , we began a thicket to be on duty in a hospital. During evening and morning rounds we had an opportunity to examine all integuments of sick people of different branches (allergological, neurological, profpatological, gastroenterological, urological, etc.).
After receiving of the degree of the candidate of medical sciences we had more free time. Therefore began to recheck the confinements and conclusions concerning of demodecosis by setting of purposeful antiparasitic treatment to 49 gastroenterological patients with accompanying clinical displays of demodecosis and to members of their families.
For the final proof of demodecosis presence it was necessary to lead clinical experiment. On August, 10th, 1980 the material was taken from the patient with discoid red lupus from the center of affection, whence were allocated demodexes in a plenty, we have processed our body. Demodecosis has taken root at once. In four months we had blossoming progressing demodecosis. By this time we have learned to define visually precisely a degree of affection of a skin by demodexes.
In January 1981 we have officially informed on results of not scheduled researches a management of the SRI of the Regional Pathology in which worked as already senior scientific employee, hardly later - in writing Minister of Healthcare of the Republic, Chairman of Scientific Medical Advice (SMA) of the Ministry of Healthcare (MH) sent us to republican Dermato-Venereologic Institute (DVI) for the proof of our scientific position.
In conditions of a hospital and dispensary DVI at all patients whom we selectively selected on clinical attributes of presence at them demodectic acariasis, from pathologically changed sites of a skin we made a fence of a material for microscopy. Microscopic research was spent by doctors-laboratory-assistants DVI. In all preparations they found out demodexes at different stages of development.
For continuation of researches on demodecosis the management of SRI of the Regional Pathology has released us from the basic work and has allocated necessary means. We carried out purposeful re-examination the received before results on the basis of many establishments of Almaty. Works were spent in hospitals of clinics and medical SRI, in city and regional adults and children's polyclinics, city Dermato-Venereologic Dispensaries (DVD), school and preschool institutions, colleges, high schools, etc. In our work took part doctors of the listed establishments: dermatologists, laboratory-assistants, oculists, pediatricians, therapists, and also doctors and candidates of medical sciences, scientific employees of Republican Allergological Center, SRI of Ophthalmology, the Regional Pathology, Microbiology and Epidemiology, etc. At selective laboratory inspection from skin of people with visual attributes of affection by mites and sicks of skin diseases were allocated Demodex folliculorum longus, Demodex folliculorum brevis and their colonies. In view of the data stated in the literature on moving demodexes through a surface of a skin, for search of mites in vivo on a surface of a skin we began to use an ophthalmologic slot lamp, an operating eye microscope, specially developed by us device for these purposes. On a surface of skin for the first time we have found out except for demodexes dermatophagoideses in an active condition. From this stage of research activity we began to pay attention to clinical features affection of skin mites depending on the found out sort of the parasite: demodexes or dermatophagoideses.
We went on different bus routes in places of a congestion of tourists and purposefully conducted calculation of persons with the healthy and affected mites’ skin. In this research directly participated the deputy director of SRI of the Regional Pathology on scientific work professor M.E. Zeltzer.
On the fourth month of treatment (by this time eight months has passed from the date of infection) of inoculate demodectic acariasis has developed the strongest allergic reaction which has been incorrectly interpreted by experts. This fact has served as an occasion for further closer studying mutual relation demodectic and dermatophagoidic acariases with an allergy.
In 1983 we have trained for a new profession on the allergist and dermatologist. In conditions of allergic cabinet of children's hospital and dermatological cabinet DVD Kentau of the South-Kazakhstan area we carried out direct treatment of patients with allergic and skin illnesses, on a call advised patients with an allergy in hospitals, including newborns in a maternity hospital.
In conditions of therapeutic site #2 polyclinics 4 in Almaty we studied a degree of affection by mites of the unorganized population. For studying mutual relation between acariases and rheumatic diseases we have trained for a new profession of the rheumatologist and carried out inspection, treatment and clinic supervision of patients of rheumatologic structure. Two times a week we were on duty in an emergency entrance ward or in abruption of rheumatologic hospitals # 2 where thoroughly got acquainted with results of inspection of this contingent of patients. The training for a new profession on the doctor of a cabinet of functional diagnostics has allowed us to carry out clinical survey of a skin of patients of a different structure: during electrocardiography inspections patients undressed. Influence of acariases on work capacity of a working contingent was studied in sanatorium-dispensary «Health».
All the next years of professional physician work we have sharpening the clinical methods of diagnostics and development ways of treatment acariases in view of clinical current illness in each concrete case. We fixed attention to a stage of acariasis process: initial, a stage developed and a stage of complication. In 1993-1997 we carried out acarological inspection of patients and their life with participation of doctor of biological sciences acarologist V.N. Kusov. By present time we have stopped to conduct purposeful visual survey of the open parts of a body of people. However involuntarily and painfully we pay attention to presence of the complicated stage of acariases at some kids met in transport and other public places. These facts stimulate us persistently to continue the address to the medical community, officials from medicine and to acarologists with a stated problem.
In July, 2007 on a beach of the International hotel in Turkey we have lead clinical survey of all integument of 200 people from various regions of a planet.
In July, 2008 along the line from Central Asia to France we have carried out visual survey of the open parts of a body of 1856 persons in turns, waiting room of the airports, interiors of planes; in a hypermarket Polygon and in a conference hall of University Montpellier Sup Agro.
For the expired period of all behind features of clinical displays and complications of acariases we have observed at 388 780 person. To purposeful clinical survey of the open parts of body we have subjected more than 2 million people from 14 cities of the former USSR and different points of a planet. Thoroughly demodectic acariasis, including reproduction of disease in clinic on the volunteer, has studied on 49285, and dermatophagoidic acariasis - on 12590 people. A course of natural distribution and expansion of clinic acariases has been tracked at 15722 people. Successful etiologic treatment was carried out to 8548 patients with various clinical masks of acariases. The conformity of clinical symptoms of skin affection degree by mites have checked up on 17823 affected.
The control research was surveyed in 1981 at 28 people with healthy skin.
Among laboratory methods of research on presence of mites in skin were applied
- The standard method scrapes of skin,
- Visual survey of a surface of skin in vivo by means of an ophthalmologic slot lamp, the operational eye microscope, portable device developed by us (Zhaxylykova and Kenenbaeva, 1990).
- A provocative method of revealing of colonies of mites in thickness of a skin (Zhaxylykova and Malikov, 1982).
- A provocative method of revealing of colonies of mites in thickness of skin with the subsequent isolate of their contents on D.K.Poljakov's method (Zhaxylykova and Malikov, 1994).
RESULTS
We studied acariasis by the non-scientific plan. Our scheduled scientific supervision was conducted for patients with chronic hepatitis in exacerbation stage and influences dietotherapy with application of national dairy products (integral mare and camel milk) on remission and current of disease. Supervision was conducted in dynamics behind a subjective and objective condition of patients, including - changes of a skin, internal bodies, clinical, biochemical and immunological analyses of blood. When it was necessary we had made radioisotopic, ultrasonic, roentgen examination in the dynamic and needle biopsy of hepar (Zhaxylykova, 1979).
The first object of ours acarological supervision was the patient, A., 48 years, with chronic persistent hepatitis in a stage of exacerbation and discoid lupus erythematosus on the face. From beet color big porous site of face skin, under the form reminding the flying butterfly, dermatologists-advisers have allocated demodexes in a plenty. On our question is she infectious for the neighbor on room dermatologists have answered negatively. This answer has seemed to us paradoxical. As so: from a skin of the patient is allocated a plenty of mites and she cannot be contagious?
During the next six years three patients with a chronic hepatites in a stage of exacerbation came on hospitalization to us. They had accompanying discoid lupus erythematosus on the face too.
Initially with these four patients closely contacted 21 people with healthy skin of the open parts of a body. Gradually we began to notice occurrence of first attributes demodecosis affections of skin. Changes progressed and finally led to various displays demodectic skin at each of them. These supervisions teach us to recognize the clinically first attributes of skin affection by demodexes.
During performance of the basic work we began to observe more closely of a skin of all patients and all people surrounded them. Involuntarily we began to apply the visual estimation of a condition of the open sites of a skin to all people surrounded us without exception. In case of detection of any changes on skin we did about it record. Those observed was appeared 317 person. As records testify, the skin of 74 % from them became affected by demodexes during 1977-1979. From the specified number for 13 people we continued to observe by 2000. The arisen changes of a skin at 10 of them we have regarded as display of demodectic acariasis II stage, and at three - III stage at them (Zhaxylykova, 1983).
The itch of skin is considered a characteristic symptom of a chronic hepatitis in a stage of exacerbation. In order to understand character of an itch at observed patients of a chronic hepatitis in a stage of exacerbation, to one patient we appointed only the standard treatment, and another to such treatment added external processing skin by antiparasitic means. For four years it collected 268 people, which had the skin affected by mites. All patients received standard therapy: a diet # 5, hepatoprotectors, desintoxication therapy, necessarily antihistamines preparations and etc. As a result of the medical treatment at all 268 people the itch decreased or disappeared completely for some time. However, at 137 of them who received in addition antiparasitic medical complex outwardly, the itch of skin stopped for a long time (more than six months), than at 131 sick of the chronic hepatitis, not received similar therapy (14-45 days). After treatment the visual condition of skin at the first 137 patients looked finer, than the skin of the other 131 persons. Thus patients were distributed in six groups. Distribution of patients by groups is shown in the table.
Table.
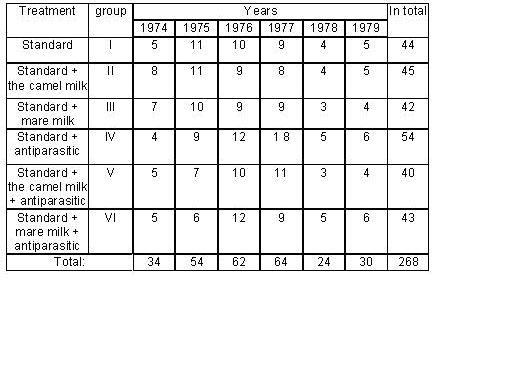
There were 44 in I-st of group, in II - 45, in III - 42, in IV - 54, V - 40, VI - 43 patients. Men - 132, women - 136. The middle age of men - 48 years, of women - 43 years. Besides, patients of II and V groups were taking whole camel milk, III and VI groups - whole mare's milk in dose of 200 ml 5 times a day before, during and after meal (depending on gastric juices acidity). In IV-VI groups patients were receiving antiparasitic medical complex outwardly.
Supervision over these patients continued from a month to two years.
Besides we carried out careful supervision over the skin of the open parts of the body of the medical personnel, visitors of hospital, friends and all met people. So our knowledge about demodectic affections of the skin of the person was perfected.
The calculation of the persons which had skin affected by the mites, in branches of RCH has shown the following. In all branches relative density of the people affected by mites was high and variation from 70 (in urological branch) up to 93 % (in allergological branch) (Zhaxylykova, 2002b).
By time of protection of the dissertation for appellation of a scientific degree of the candidate of medical sciences we have come to conclusion about presence among surrounded people contagiosity skin illness caused by Demodex mites but not consideration of clinical medicine and dermatologists (scabiologists).
In that interval of time (1979) medicine also did not assume the presence among the population of any unknown infectious illness.
The medical science seemed highly developed; the medical technique reached unprecedented heights: our clinic has been equipped by the advanced medical-diagnostic equipment. To stand out against this background the presence not diagnosed, not considered, but extending among people infectious illness - demodecosis seemed to us paradoxical.
It was the first stage of our researches.
In 1980 we have started to test the received results. For this purpose for 49 person with affected by demodexes skin an external antiparasitic treatment was provided, which led to a full liquidation of itch and distinct clinical improvement of the skin. The result of treatment objectively testified the presence at the observed the initial disease of skin - demodecosis. As a result of the medical treatment of this group of patients the former conclusions were confirmed.
For final belief in correctness of the supervision we have carried out clinical experiment - have infected myself by demodecosis. Self-experiment has gone right. Demodeсosis has taken root. The result of this clinical experiment testified the correctness of our preceded supervision and the conclusions followed from them. Our conclusion was the following: demodecosis among people is present, extends like an avalanche, but by clinical medicine is not diagnosed. We do not have doubts in spread among the population extending demodecosis.
In order to have an opportunity to observe the development of the imparted illness we got over for work the senior scientific employee in a leading research institute, have taken the permit on four-month specialization (from September till December inclusive) on therapy (during study more free time is available). In January 1981 after study we have returned for work and have first of all informed the head of department (it is the deputy director of SRI of the Regional Pathology on scientific work) on results of experiment and the firm conclusion about the found out new phenomenon - presence of unrecognizable by clinical medicine infectious illness - demodecosis. Later about the same we have informed also director of institute with a detailed statement of the known scientific literature and the facts received during supervision. In many respects director of institute agreed with our reasonings, marking their conformity to aggregate biological laws and it encouraged us. During trips on a municipal transport and visual review of persons with the changed skin the deputy director professor M.E.Zeltzer asked different questions, answers on which it was necessary to find out during forthcoming researches.
Nobody released us from work of that we have carried out self-experiment. We did not have time for observance of a correct mode of rest and nutrition, qualitative carrying out of treatment. On ourselves we developed treatment imparted demodecosis. Probably, not all used medical procedures were correct. But all these moments has an influence on our general condition. Can be therefore during treatment at us has developed the hardest allergic reaction, accompanied a massive oedemata and reddening of all skin. On sites with a gentle skin (necks, axillary, underknee, inguen, elbow bends) have arisen bubbles which were opened and gave madidans and burning. As any doctor of that period we were frightened with outright developed allergy. Therefore we have addressed for advice and help to the main dermatologist of Republic to professor [R.K.Makasheva]. First, she has not believed to our statement that demodecosis has imparted on us. Secondly, on our twice asked direct question «Am I infectious?» she has answered negatively. But her eyes said for ten present doctors-cadets, that with colleague (i.e. with me) happened slightly wrong. (Among doctors-cadets present on that advisory reception many still should be alive.). Answers of the professor once again testified, that demodecosis in medicine is unknown and allergy is interpreted incorrectly. The professor has written out a direction on urgent hospitalization in DVI with the diagnosis «Erythrodermia».
Direction on the hospitalization, which has been written out by the professor, and her answers to asked questions together with the request to hospitalize in our branch, «if I am not infectious», have been transferred to the head of department of SRI of the Regional Pathology who, having burst out laughing, has recommended to address in a regional polyclinic for a hospital leaf for treatment in-home. The divisional dermatologist has written out to us a leaf of invalidity with the diagnosis «Drug dermatitis». Thus for the first time we have learned about the attitude of demodecosis to an allergy. Since this period we began to search more carefully for any allergic displays at patients with demodecosis on their clinical condition, results of laboratory and tool researches. In order to find out, was our condition infectious, a peel strewed from our skin, we have collected on a sterile bed-sheet and have kept in it wrapped up two prepared kittens within an hour. At both kittens has developed typical, described in the veterinary literature, demodectic process with primary affection of face skin - on one, body skin – on the other cat. Hence, demodecosis, diagnosed at the described stage experts as erythrodermia and dermatitis, was infectious. It is necessary to note, that both of the expert on a clinical condition of our skin have truly diagnosed erythrodermia and dermatitis. So it is many-sided demodecosis. The clinical condition of skin varied quickly. If in first half of day during consultation of the professor the skin had one clinical picture (the diagnosis erythrodermia) in second half of the same day during survey by its divisional dermatologist the skin looked absolutely differently (the diagnosis - dermatitis). Unique medical action which we have lead between these two surveys - have accepted an injection 2 ml solution of Clemastini and per os - one tablet of Suprastin (Chloropyramine).
As acariasis always begins with affection of skin and imparted with an environment mucous its clinical diagnostics does not difficulties. By this time we have learned to define visually precisely demodectic acariasis. During this period we had been developed new ways of diagnostics demodectic acariasis and also the convenient device for realization of one of the ways of diagnostics of acariasis.
To our institute MH of Republic did not allocate financing on theme of demodecosis. Therefore we have addressed with a statement of the revealed fact to Minister of Health Kazakh SSR. Chairman of SMA MH has directed us in Republican DVI «for the proof of our scientific position».
In conditions of DVI hospital and dispensary we extracted the contents of the pathological elements of the skin of patients from the most various places of their body. The microscopy research of preparations was made by doctors-laboratorians of this institute. They found demodexes at different stages of development in all preparations. Diagnoses of patients at which the fence of a material was made, were the most different: widespread pink lichen, psoriasis, lichen chronicus simplex, prurigo, dermatitis, lichen ruber planus, etc. On advisory reception in DVD DVI some patients has obvious clinic and anamnestic displays of demodecosis, confirmed discover demodexes from pathological elements of their skin. For example, at the girl of 16 years complained an itch and efflorescence have bright red papula rash on different sites of a body. One day prior of the described reaction she has the first in a life intimate contact with the guy. The guy has red acne on the face. The girl, not embarrassed, has told that the guy kissed all of her body. In preparations from a material taken by us from different sites of her body, laboratorians of DVI have found out demodexes. However dermatologists-advisers have drawn the conclusion «Acute urticaria» and have sent the girl on cure in a regional polyclinic. Other case: the father comes with six-year son on consultation of complaints to full loss of eyelashes and eyebrows at the boy. Clinically we saw blossoming demodecosis both at the father, and at the son. Therefore we asked to take analysis from both. The doctors-laboratorians have found out demodexes with that difference: from a skin of the father have chosen Demodex folliculorum, and from a skin of area of eyebrows of the son - Demodex brevis. However dermatologists-advisers have appointed endocrinology inspection to the boy on a residence. Such cases were much for two weeks of our combined work. However to SMA Republics MH management DVI has written the answer: demodexes is saprophyte and are present practically at all.
In Central DVI, being in Moscow, have approvingly regarded of our oral statement of a problem and have asked to send the official statement. But on the official letter of our Institute have sent the negative answer. So we have remained alone with a global problem.
We continued researches: realize mass survey for affection of skin of the open parts of a body of people by acariasis in public places. Among 2 million clinically examined there were inhabitants of Almaty, Moscow, St.-Petersburg, Kazan, Sochi, Pskov, Riga, Vilnius, Chimkent, Kentau, Tashkent, Bishkek, Ashkhabad, Dushanbe, and also the tourists who have arrived to Almaty from different corners of the former USSR, etc. 91 % examined had affected skin by acariasis of the open parts of a body. Thus, results of researches testified to a wide circulation of acariasis among people. And results of this survey on months within the same years testified the growth of morbidity. So, in January, 1981 among 18070 examined 27 % had healthy skin. With each month the quantity of people with a healthy skin of the open parts of a body decreased. In August from among 23175 only 0,2 % had a healthy skin (Zhaxylykova and Zhunusova, 2001). Last person, who had healthy skin, was the tourist from Western Siberia (we have approached to him and have asked, from whence he is arrived).
Considering the microscopic sizes of demodexes, described in the literature features of their biology, use of increasing devices in ophthalmology, we began to apply to detection of mites on a skin of patients in vivo an ophthalmologic slot-hole lamp. We have seen on a skin of the persons both alive demodexes and alive dermatophagoidesses for the first time. In a sight demodexes had a long body with cross-section draw a back half. They have been turned by a head to an input in hole of a channel of skin gland. At patients with acne illness in plentiful liquid grease separated skin demodexes freely floated, reminding tadpoles in water. Dermatophagoidesses had a short volumetric body with translucent vertical as sail a back part of body. Color of a chitinous cover of mites corresponded to color of a skin of the patient (Zhaxylykova, 1992a). In operational unit SRI of Ophthalmology on an operational eye microscope with participation of professors-oculists of T.S. Teleuova and V.G. Uldanov carried out survey of a skin of patients of various branches of this establishment and the patients invited from polyclinic.
Since this period we began to study features of changes on a skin of patients at presence at them dermatophagoidesses. In practice dermatophagoidic acariasis in most cases accompanies with demodectic acariasis. Clinically (i.e. visually) at many patients is available combination invasion by demodexes and dermatophagoidesses, sometimes - sarcoptids and other mites, not counting bacteria (staphylococcus, streptococcus), viruses, fungis, etc.
Within two years, receiving both the material and moral help and support from the direction of SRI of the Regional Pathology, we continued our researches on the basis of different establishments of Almaty. In parallel we developed the medical treatment of the inoculate demodecosis. We acquainted widely with the literature on various branches of the biology having any attitude to acaries (acarology, parasitology, veterinary, zoology; microbiology, dermatology, allergology and other branches of medicine). We did repeated attempts to come into contact to experts’ dermatologists and allergists, including specialists of Moscow. But contact has not take place. The reason of it became known to us only after collapse of the Union. To get a job the allergist and dermatologist we move at own expense to the remote city of Kentau per 1982.
We were trained on the allergist in conditions of Institute of improvement of doctors of Kazan, on dermatologist - in the Sochi SRI of Balneology. In a Kentau on a post of the allergist of a children's polyclinic and dermatologist of the city DVD we began to treat sick people by our methods with taking into account of installations in medicine and current legislations. We received striking results: the sick people who has gasp for breath in conditions of Kentau after our treatment freely breathed. Not capable to move and work because of skin problems on the legs, after our several medical procedures came back to former workplaces, etc. What else the proof in correctness of our professional position is necessary?
We have returned in capital. In the past year both Minister of Health of Republic and chairman of SMA of MH were replaced. Therefore we got fixed up in a job in a city polyclinic 4 again as the district therapist and after corresponding specializations worked as the rheumatologist, then as the doctor of a cabinet of functional diagnostics. Rheumatic diseases are the one of the clinical masks of acariases. Therefore we worked as rheumatologist and two times a week were on duty in the republican rheumatologic center. During evening and morning detour had an opportunity to examine all skin of patients. It is necessary to emphasize, that in conditions of a polyclinic we had to appoint patients treatment within the limits of standard in medicine. But under the consent of separate patients we introduce the corresponding correction into their treatment and received their gratitude. Patients undressed in the cabinet of functional diagnostics. The nurse carried out procedure of inspection; we studied an integument of the patient. The effect of acariases on a health of a working contingent we have tried to study in conditions of sanatorium "Health ". At 78 % from them of the manifestations and complications of acariases was a principal cause of their stay in a health resort. I.e. the most directed diagnosis was either manifestation or complication of acariasis.
Among inhabitants of a medical site of №2 of polyclinics №4 of Almaty were not persons not affected by mites. All 319 dispensary patients of rheumatological cabinet suffered by acariasis in a stage of complication. From 18700 patients who have been inspected in a cabinet of functional diagnostics, at 40 % is revealed initial, at 52 % - a stage of the developed disease, at 8 % - the complicated stage (on our classification) of acariases (Zhaxylykova, 1999). During 1991-2006 specific gravity of patients with an initial stage of acariases, addressed the help to allergologist, has decreased with 91 up to 12 %. The percent of patients with various complications of acariases has accordingly increased. Per 2006-2008 is marked the growth of a number of patients who addressed with heavy and heaviest complications of acariases (Zhaxylykova et el., 2008).
With 1979 for 1996 we studied all accessible literature having any possible attitude to mites and diseases, them caused, in biology, medicine, parasitology, veterinary science, acarology, zoology, microbiology in libraries of cities Almaty, St.-Petersburg, Moscow. We have found in them almost all about acariasis in parts. Without their data we could not so is thin to understand in unique unusual supervision and to be assured in absolute correctness of our conclusions. Also a considerable role has played our interest in student's years to ophthalmologic operations, the experience of work in the beginning of medical practice in conditions of the remote medical sites, scientific activity on the basis of gastroenterology branches of technically highly equipped clinic.
It is necessary to note, that in conditions of polyclinics and hospitals always there was a full opportunity to appoint patients necessary inspections.
At purposeful research of a skin 17823 affected in 98,1 % are detected demodexes, in 0,5 % - dermatophagoidesses, in 0,6 % of cases were found out sarcoptids, and in 0,8 % - other mites (onions, grain, granary, paunchy /predatory/, root). Several kinds of mites was finding in 2, 4 % of researches. Among 107 affected (0,6 % investigated) with presence Sarcoptes scabiei at 39 person mainly on a skin of face were marked precisely visible scabby courses and there was an itch. Specific identification of mites was spent by Dr. Sci. Biol, acarologist V.N. Kusov. The imago, larvae forms and eggs of demodexes were found out in 100 % of cases in a near wall material at research of contents of papule at 242 people with various itching diseases of skin, acne elements at 247 people, atheroma - at 18, chalazion - at 12 patients. Within 18 years to us refer on reception 14 patients with a classical itch. At one of them the itch of skin has not disappeared after usual treatment of sarcoptosis. At four patients the itch of skin disappeared in first days after treatment but has renewed again within 4-9 days and slowly amplified. Only after carrying out purposeful antidemodectic treatments the itch of skin at all five patients has completely stopped. From among patients who have addressed to us with chronic itching diseases of skin (eczema, lichen chronicus simplex, prurigo, etc.), at 23 patients from skin was allocated Sarcoptes scabiei. All of them until addressed to us during from 5 months till 8 years received ineffective treatment at dermatologists and allergists in polyclinic and stationary conditions.
Results of the lead researches and conclusions following from them were divulged in the oral and written form to Ministers of Health of Republican and Union level, chairmen of SMA of Kazakhstan and the Union, managers of Republican and Central DVI, Center of Allergology, Institute of Rheumatology, etc.; at medical conferences, Congresses and Symposiums of Republican, Union and International level which are passed in Almaty; sessions of Societies Dermatologists and Allergists of Almaty, All-Union conference of Acarologists in Frunze in 1986, etc. During this period on the background of practical absence of the wide information on an epidemiological situation on the planet our data about presence of non-registered by the clinical medicine infectious disease among people has been accepted ambiguously both officials in the field of public health, and specialists - dermatologists and allergists.
At all 200 people having a rest on a beach in Turkey the skin has been affected by mites. Among them unusual displays acariases, differing changes from affection of skin by mites in other regions, took place at inhabitants of the Scandinavian countries. Among 1856 person, examined in 2008, people with healthy, not affected by mites skin of the open parts of the body were not. At that the initial stage of acariases was present only at 240 (13 %) from them. At two people we were inclined to think of presence of III stage of acariases. At the others acariasis was in the developed stage.
Among successfully treated patients with acariases up to address to us doctors had been established following diagnoses: allergic blepharo-conjunctivitis - at 86 people, pterigium - at 11, arcus senilis - 3, chalazion - 9, ectropion - 1, xanthelasma - 7, an allergic all-the-year-round rhinitis - 178, polynosis - 471, food and drug allergy - 763, acne illness - 761, atopic dermatitis - 712, eczema -149, acute urticaria - 42, chronic relapse urticaria - 114, widespread dermatitis - 912, lichen chronicus simplex - 179, contact dermatitis - 255, rosacea - 23, rhinophima - 19, local dermatitis - 972, psoriasis - 117, parapsoriasis - 72, prurigo - 27, lupus erythematosus - 49, photodermatosis - 43, furunculosis - 11, bronchitis asthmaticus - 12, verruca plana - 24, scab - 14, cellulitis - 12, dryness of a skin - 18, erythema nodosum - 23, rheumatism - 24, Quincke's edema - 14, mastopathy - 7, hemorrhoid - 6, morphea -7, morphea linearis an initial stage - 2, vitiligo - 17, precancerous conditions of a skin - 13, Cancer of a skin - 7, kraurosis vulvae - 14, leukoplakia - 7, alopecia - 36, local syndrome of a languid skin - 2, delirium of parasitosis - at 3 persons, etc.
In people with healthy skin mites in skin not found any of accessible methods of diagnostics.
DISCUSSION
In the given work we considered correct to discuss mainly acarological aspects of a stated problem as given clause goes to a press in Journal of Acarology.
Casual detection demodexes of a plenty in a skin of the observed patient with a pathology of a hepar has caused in us, as the medical worker, epidemiological vigilance. As gastroenterologist and the therapist we did not know about the opinion which has fixed in dermatology occasion of a saprophyte role of demodexes. Therefore the fact of allocation from a skin of our patient mites Demodex, we have apprehended under laws of epidemiology and have begun own researches. A chance or a law, but our clinical supervision has coincided with intensive distribution demodecosis among the population. Since this period on statistics of specialists is observed rapid growth of allergic and skin illnesses. On our rechecked data allergic and skin illnesses are the most frequent early clinical masks of acariases (Zhaxylykova, 2000).
On a question «Demodex is saprophyte or parasite?» after long-term researches we unequivocally answer: «Demodex is the parasite». We emphasize: our data do not contradict the facts stated in the scientific literature. Even if 167 years ago Demodex was the symbiont of the person but for such long period of symbiotic cohabitation, according to laws of biology, it could pass from ectoparasite to endoparasite way of life (Roitman and Beer, 2008). And the last centuries, and now failures in treatment of skin patients lesion with demodexes are connected with a lack of knowledge of clinic of demodecosis and inability correctly to medically it. Treatment of demodectic acariasis differs from treatment of sarcoptic a little.
Parasitism of Gamasidae mites living now in a household dust, is at a stage of becoming about what allow to judge relative more easy clinical expansion caused by them acariasis, weak contagiosity, speed of treatment. Acariases, caused by these mites were characterized by more rare papule efflorescences in the sizes in 3-5 mm in diameter. Color of these elements coincided with color of a surrounding skin. The itch of a zone of the affection, amplifying during evening and night time, at them was present. For example, from the patient with mites dermatitis, caused by predatory mites, the husband was infected with in a month. Antiparasitic treatment has quickly helped. From skin 142 affected are excreted onions, grain, granary, big-bellied /predatory/, root. But in a dust of living rooms of some of them prevailed chicken mites Dermanyssus gallinae (Zhaxylykova and Kusov, 2001).
Mixed infection by demodexes and dermatophagoidesses at sarcoptic acariasis was and remains. Hence, the classical scab is caused by association of these mites with prevalence Sarcoptes scabiei. Sarcoptids lay passage in superficial layers of a skin, but in end of XX century ascertained that it layers in skin more deeply. Representatives of all three sorts of mites (Sarcoptes, Demodex, Dermatophagoides) were found out in times of a skin glands though glands of skin considered as a favourite place of dwelling of demodexes. There are a lot of glands in a skin of the person. They have a different structure, depth of lie, length, width and the form of terminal channel. There are data of some authors who approve, that Demodex is capable to make courses in a skin. Deep layers of a skin are considered as a place of localization Dermatophagoides. Proceeding from a place of dwelling of each of the listed sorts of mites, medical influence on each of them should be a miscellaneous. The medical procedures spent at treatment of a classical itch, influence within the limits of superficial layers of a skin. Access of scabicids up to deep lying glands of skin with twist channels is not provided. Mites who live on top level of an integument therefore perish. The mites which have remained in deeper layers of skin (dermatophagoidesses, in complex glands - demodexes and sarcoptids) do not perish. At patients does not occur full disposal of the scabby mites. After course of treatment sarcoptic acariasis the itch of skin stops or sharply decreases in the first days. In most cases the itch of skin renews in accruing rate of proportionally intensity of reproduction in quantity and settle of the remained mites. For this reason after treatment of a classical scab of patients continues to disturb weak intensity itch and dryness of a skin. Hence, so-called acarophobia and a residual itch actually are caused the continuing invasion skin of the patients by demodexes, dermatophagoidesses and remained in deeply located glands of skin sarcoptids. The problem acarologists to help doctors with diagnostics of this conditions. Involuntarily there is a question: why not relapse the sarcoptic scab? In some cases it relapses. But more often sarcoptids remains a little. Symbiosis of demodexes, dermatophagoidesses and sarcoptids are proceeds, but already at other quantitative parity than before treatment of a classical scab. Contagiosity of Sarcoptes scabiei goes down, as under laws of biology at symbiotic residing demodexes, dermatophagoidesses and sarcoptids controled number and virulence (pathogenicity) each other. Therefore in a clinical picture of illness at such patient symptoms of sarcoptec itches do not prevail. In case of detection Sarcoptes scabiei in skin of "practically healthy" people because of ignorance of clinic present of demodectic and (or) dermatophagoidic acariasis the patient consider as the healthy carrier of sarcoptid. That is why in our supervision in all cases of allocation from skin Sarcoptes scabiei purposeful etiopatogenethic treatment led to full liquidation both objective and subjective displays of illness. On the basis of the stated data we consider, that in all cases so-called «healthy carrier of scabby mites» takes place demodectic and (or) dermatophagoidic acariasis with participation Sarcoptes scabiei. Hence, acarotregerstvo - an inadmissible condition in clinical and epidemiological aspect (Zhaxylykova, 1999). Sarcoptids lay passage in superficial layers of a skin, but in end of XX century ascertained that it layers in skin more deeply. Representatives of all three sorts of mites () were found out in times of a skin glands though glands of skin considered as a favourite place of dwelling of demodexes. There are a lot of glands in a skin of the person. They have a different structure, depth of lie, length, width and the form of terminal channel. There are data of some authors who approve, that is capable to make courses in a skin. Deep layers of a skin are considered as a place of localization. Proceeding from a place of dwelling of each of the listed sorts of mites, medical influence on each of them should be a miscellaneous. The medical procedures spent at treatment of a classical itch, influence within the limits of superficial layers of a skin. Access of scabicids up to deep lying glands of skin with twist channels is not provided. Mites who live on top level of an integument therefore perish. The mites which have remained in deeper layers of skin (dermatophagoidesses, in complex glands - demodexes and sarcoptids) do not perish. At patients does not occur full disposal of the scabby mites. After course of treatment sarcoptic acariasis the itch of skin stops or sharply decreases in the first days. In most cases the itch of skin renews in accruing rate of proportionally intensity of reproduction in quantity and settle of the remained mites. For this reason after treatment of a classical scab of patients continues to disturb weak intensity itch and dryness of a skin. Hence, so-called acarophobia and a residual itch actually are caused the continuing invasion skin of the patients by demodexes, dermatophagoidesses and remained in deeply located glands of skin sarcoptids. Involuntarily there is a question: why not relapse the sarcoptic scab? In some cases it relapses. But more often sarcoptids remains a little. Symbiosis of demodexes, dermatophagoidesses and sarcoptids are proceeds, but already at other quantitative parity than before treatment of a classical scab. Contagiosity of goes down, as under laws of biology at symbiotic residing demodexes, dermatophagoidesses and sarcoptids controled number and virulence (pathogenicity) each other. Therefore in a clinical picture of illness at such patient symptoms of sarcoptec itches do not prevail. In case of detection in skin of "practically healthy" people because of ignorance of clinic present of demodectic and (or) dermatophagoidic acariasis the patient consider as the healthy carrier of sarcoptid. That is why in our supervision in all cases of allocation from skin purposeful etiopatogenethic treatment led to full liquidation both objective and subjective displays of illness. On the basis of the stated data we consider, that in all cases so-called «healthy carrier of scabby mites» takes place demodectic and (or) dermatophagoidic acariasis with participation Hence, acarotregerstvo - an inadmissible condition in clinical and epidemiological aspect (Zhaxylykova, 1999).
It is established that mites carry by on a surface and inside of the body of smaller, than they, microorganisms - bacteria, viruses, fungis, eggs of helminthes, etc. Need be imagined how much diverse there can be this associative complex from community of mites and the listed microorganisms. Here it is necessary to add and features of each macroorganism with its anatomic, biochemical, immunological, psychological and other features; food, labour, household, weekend and other habits; influence of natural-climatic factors, etc. All of them leave traces on the further stay of community of microorganisms in a body affected and finally - on a condition of its health. That is why acariasis is clinically shown differently at different people, including at members of one family. For this reason acariasis is many-sided. As a matter of fact any displays of acariasis are infectious. But after infection at each concrete person acariasis is shown differently, therefore contagious illnesses obviously are not noticed both researchers, and inhabitants. On the other hand at identical household, alimentary, industrial, weekend and other conditions related organisms are capable to react identically at affection by an identical associative complex of activators. The given situation declines researchers to think about hereditary the caused conditions and illnesses though actually illnesses are transferred at close contact. In practice it is too much cases when in families for the first time find out the illnesses which are considered in medicine is hereditary caused. Thus researchers and patients are compelled to sin on ecology. Actually the ecology in such situations plays only small role (Jusupova et al., 1995). The problem of acarologists together with microbiologists by allocation of an associative complex of activators to prove contagious character of illness in such situations.
In the medical literature published a lot of works about «illusions of parasitosis». All patients with such diagnosis complained not simply of an itch of skin, but also on feeling of crawling of an insect on and in a skin, feeling a touch of down, hair to a skin, feeling thrust a needle in a skin and deeply located fabrics, etc. As authors from the different countries write, that among these patients there were also doctors. Because of absence of exact laboratory diagnostics to these patients did not trust and quite often placed them in psychiatric hospitals. Actually it is very sensitive people having too affection by mites an organism and environment. To us for 18 years have addressed three patients with «delirium of parasitosis». In these three cases of conditions of their skin of patients we described a condition of their life and health of other members of their families. Those patients confirmed it with surprise. After realization of our recommendations the condition of all patients has improved. One of them has completely got rid of illness because he had an opportunity to pass all the appointed courses of treatment. To us addressed patients who complained of an itch inside of a thorax, in thickness of muscles of a hip, inside of bones of a shin, etc. We surveyed them accessible modern laboratory-tool methods, carefully watched liquidation of these symptoms during treatment (Zhaxylykova, 2007a). The doctor always should trust patients, but, trusting, always to check. Such cases - one more point of the appendix for teamwork for acarologists and scientists-physicians.
On the one hand acarologists all of the world ascertain about increase in the species and quantitative attitude of mites in the nearest environment of the modern person. But in the medical reality this fact almost has no practical exit. On the other hand the WHO informs that health of the modern person on 50 % depends on conditions and way of life. Its are right both those and others. But they work is separated. Despite of ascertaining by acarologists about growth of pollution of the environment of the modern person by increasing quantity of specieses and individuals of mites in medicine corresponding recommendations on elimination of family life are given only to asthmatics. The population does not know about necessity of carrying out antiallergic elimination of life from mites. Such recommendation would be the most effective preventive of acariases with their various clinical masks, including allergy and allergodermatoses. Certainly conditions of places of stay stuffed by mites directly influence health of the modern person (Zhaxylykova and Seisenbaev, 2002; Zhaxylykova et al., 2008). Only joint efforts acarologists and physicians can develop correct recommendations on clearing places of stay of people from mites.
It is necessary to give due to those who lets out domestic appliances, bedding, clothes, etc., intended for reduction of mites in an environment of the person. However the let out goods and devices not always correspond to the applicability. All of them are very necessary to people, but without direct participation of acarologists and clinical physicians in creation of the similar goods and devices a problem not to solve correctly.
There was an opinion among the dermatologists that demodexes crawl out from the glands to the skin surface to lay eggs and then again crawl back to the skin pores. Such an opinion was published in the medical literature. Such a behavior does not go in line with the incredible adaptability of mites and ability to reproduction and survival. But most part of expert found out that demodexes settle on the skin surface and live in colonies in their habitats. The structure of such colonies are described in details. On the outer part the colony is hemmed with the connective tissue capsule, which is a relatively thick-walled bladder, which protects the organisms of the master from the antigens of the mites. Thickening the capsule of the affected by mites gland the microorganism in its way protects itself from undesirable cohabitants. On the inner part close to the wall of the capsule of the colony there are active individuals of demodexes at the stages of imago and nymph-2. Deeper there are immobile stages: eggs, maggots, nymphs-1. In the center there is a homogeneous caseous mass, representing the decayed remains and excreta of the perished mites, cast-off epithelium, gland’s secretion. In our work we were convinced in correctness of such a description (Zhaxylykova, 2007b). Unfortunately, in practical healthcare sampling to check the mites presence is made incorrectly. We saw many medical institutions where scrape from the skin is made with the surgical scalpel and not with Folkmanne’s curette. In such an examination they get only the middle content of the colonies or the outer skin epidermis, which has no mites. The result of such an examination is always negative, because the mites’ colonies are not extracted for examination. Glandular tissue is present in the human organism not only in the skin but also on the mucous tunics, serous tunics, and fatty tissue. Some internal organs and tissues have glandular structure. Dissemination of demodexes on the animals’ organisms is made by lymphatic tracts and fatty tissue. The task of acarologists is to work out the methods of finding mites not only in the skin glands but also in the glands of the organs and tissues of people.
Taking into account the immune status of the organism affected by mites we developed a method allowing making visible the places of mites colonies location in the skin. For that we provoke local allergy reaction, as a result of which the walls of the affected skin glands allergically swell. After that the colony is visible together with the orifice of the excretory gland tract. Further one can make husking of the near-the-wall content of the colony with a thin Folkmanne’s curette. In such materials we can always find demodexes at different stages of development. Patients with prurigo, acne, neurofibromatosis, hemangiomatosis, poliposis, hemorrhoids, etc. we can husk the near-the-wall content of the visible knots without provoking and find in them colonies of mites (Zhaxylykova, 1992a). Based on 100% discovery of mites in the provoked colonies it is possible not to conduct the second stage of this method. It is possible that such colonies are inhabited not only by demodexes. It’s only in hands of acarologists to clarify the situation.
Based on the scientific literature dermatophagoideses cause dermascab itch. It was believed so 145 years ago. Nowadays dermascab itch is not diagnosed. Scientists state that dermatophagoideses live in the bedding and eat the cast-off epithelium of the human skin. They even calculated how many grams of the epithelium one mite can eat during the day, week, month. If dermatophagoideses eat only the old epithelium of the human skin then it looks like they are useful to people cleaning their beddings from the skin waste. That is they are paramedics of our beddings. The same we could tell about demodexes in regard to our skin, if they really eat only the content and the cast-off epithelium of the skin glands walls. Unfortunately, it is not so. Acarologists write that demodexes are able to pierce the walls of the cells of the master with chelicera and suck their content. When describing the demodexes anatomy cause dermascab itch. It was believed so 145 years ago. Nowadays dermascab itch is not diagnosed. Scientists state that dermatophagoideses live in the bedding and eat the cast-off epithelium of the human skin. They even calculated how many grams of the epithelium one mite can eat during the day, week, month. If dermatophagoideses eat only the old epithelium of the human skin then it looks like they are useful to people cleaning their beddings from the skin waste. That is they are paramedics of our beddings. The same we could tell about demodexes in regard to our skin, if they really eat only the content and the cast-off epithelium of the skin glands walls. Unfortunately, it is not so. Acarologists write that demodexes are able to pierce the walls of the cells of the master with chelicera and suck their content. When describing the demodexes anatomy the literature shows strong piercing-cutting-gnawing and sucking mouthparts. Judging by many objective characteristics we are prone to think that demodexes and dermatophagoideses eat the blood and tissues of the master’s body. For instance, we can judge about it by the presence of not rarely met anemia of the affected by acariasis, minus tissue in case of stretch marks, scleroderma, etc. We treated a boy, whom dermatophagoideses just ate a piece of the left auricle in the form of triangle with the top directed to the acoustic duct. We had an elderly patient with a deep infected ulcer of the left temporal area caused by demodexes. In the course of treatment of the demodectic acariasis stretch marks and scleroderma focus experienced involution (Zhaxylykova, 2002a). There is a lot of such examples. The clinical data dictate for necessity of recheck of similar changes both in cases of invasion of dermatophagoideses and demodexes.
In the course of examination of the affected and their way of life we met a fact, which we cannot explain. From the pathologic elements of the skin of patients with allergic dermatosis from different part of the bodies we found demodexes. When examining the dust from their homes we could see dermatophagoideses so mobile and numerous that reminded a flock of sparrows. It looked like they will jump out of the Petri dish onto the researcher. Only in one case in the dust from a cabinet we found a dead individual of demodexes (Zhaxylykova, 2006a). The question is why in the patient’s skin only demodexes are discovered, and at home – only dermatophagoideses? Only acarologists can clarify the situation.?
No one has ever studied how demodexes and dermatophagoideses behave in the human organism. But nobody looks for dermatophagoideses on the skin, on and in the mucous tunics, not talking about organs and tissues. Such a study was not given to sarcoptids, either, which by the descriptions in the literature in the worst cases also cause various clinical masks that go beyond the toxic syndrome. Our clinical observations testify that demodexes and dermatophagoideses affect internal organs and tissues of a human, which can be clearly traced by the dynamics of complaints and objective data of the treated. How do the demodexes and dermatophagoideses look after long stay in the internal organs and tissues? This task can be solved only by acarologists, as the mentioned mites after long stay in the internal organs and tissues like Linguatula serrata can change their appearance beyond recognition. Immunologists have long ago been writing about the adaptive change by the parasites of their structural tissue components in harmony with the master’s tissues (Khaitova, 2002).
Seeing is believing. Observed in the natural conditions numerous facts do not allow us agree with the existing theoretical situation in the medicine. We dedicated our medical activities to study of acariases, repeated check of stated in these work facts, development of treatment of various manifestations and complication of acariases (Zhaxylykova,2006b).
An observation, which started with a casual fact, then revealed an avalanche propagation of demodectic acariasis among the population. Besides the demodectic one some other acariases, such as dermatophagoidectic, sarcoptic and so on, appeared to be rather widespread. In this process, other house dust mites of a modern person also start to take a direct part.
Acariasis is a primary-chronic infection. Due to the absence of proper fighting various clinical masks of acariases are registered in medicine as allergic reactions, allergic, skin, rheumatic, oncological and other widespread primary-chronic illnesses of people. Connecting together the two mentioned facts (presence of acariases and their clinical masks in the form of NID) we can theoretically suppose presence of the pandemic of acariases on the planet. We have conducted a mass clinic research as well. We have examined a great number of people, of whom 91% had affected by mites skin. Starting from 1982 among the clinically examined, we did not meet people with healthy skin. Every year we had to state the reduction of acariases at the initial stage (Zhaxylykova 2007c). Finally, in July of the last two years we purposefully conducted clinical examination of 2056 persons from different places of the world. Among the examined, there was no one with healthy skin, free from acariasis, but acariasis of II stage was already prevailing. Thus, pandemic of acariases is clearly seen. In the current situation, one can find mites on and in the bodies of people. Available methods of diagnostics are obsolete, they are not conducted accurately, that is why the percentage of discovery of mites on the human skin is low and does not correspond to the reality. New efficient methods are not developed, and the developed ones are not widely introduced into the medical practice. That’s why the mites are discovered not in all the cases of acariasis affection of skin. Studied by us clinic of acariases is not used by the clinic medicine. Diseases caused by demodexes, dermatophagoideses and sarcoptides are not studied enough and correctly in the medicine. Without participation of acarologists the medicine will not establish the truth of presence of pandemic of acariases. In its turn universal affection by acariasis cannot help but reflect on the clinical course of the known infection and non-infection diseases of people. However, it does not mean that acarologists should start examining people. They can independently examine prosector and operation materials. In our century, when doctors trust the results of laboratory and tool researches more than their own sense organs, participation of acarologists in examination of patients together with laboratory doctors is extremely necessary. Moreover, the patient of the XXI century is competent, and would like to know the cause factor of his illness. That is why it is so necessary to introduce highly informative acarological methods of diagnostics in medicine. Only acarologists can help in achieving it.
Time and practice proved our rightfulness. Acariases are clearly diagnosed clinically. Their manifestations on the skin and visible mucous tunics can be seen. Therefore in 2000, we for the first time published web site providing the main aspects of this scientific work in Russian. The same year we sent the information in English by e-mail to several representative offices of WHO, associations of dermatologists, allergologists and acarologists of many countries. Since 1981, detailed information was disseminated on the territory of the former USSR. But interest of doctors of the world to the mite pathology of a human does not comply with the requirements of reality. So with the aim of informing the acarologists about the existing situation in medicine with the acariasis we participated in the VI Congress of the European Association of Acarologists (2008).
The biotope of modern human is full of hordes of mites – and this is already an irrefutable fact. But at the same time no one examine foodstuff, ready and cooked in advance food, which the mite can not miss with the existing situation in the biotope, full of mites everywhere in the world (Sergiev, 2006; Vasilyeva, 2006). + 5ºС (this is the temperature in the refrigerator) is not an obstacle for mites, if they are able to live even in a bottle of wine, at the foot of volcano and so on.
Habit of the micro world is best known by the acarologists and microbiologists. What do the cockroaches do when all of a sudden someone take away a paper under which they hid, - everyone can see well enough. But what is the behavior of mites in such a situation, when someone tries to find them in the organs, tissues, secretions of people? As the Chinese scientists say lice leave the body of a hopeless patient. How do mites behave in such a situation? Competent surgeon ablates a cancer tumor so that after the operation the patient had no metastases through his fault. What is the right way to make an examination so that the mites, which have eight legs, get under the microscope together with the examined material, and will not have time to escape? More questions than answers. We should answer them together. But a general practitioner should first of all know the clinical methods of diagnosing acariases. So far we only visually (that is clinically) can recognize acariases. That is why the answer «negative result of a laboratory research is a result anyway» can be good only for us but not for those who is doubting presence of the pandemic of acariases on the planet (Zhaxylykova, 2006c).
Our position is proved by time and practice. We do not suggest a next theory in medicine. We offer radical methods of medical treatment and prevention of allergic dermatoses, which are the earliest and most frequent clinical masks of acariases. To develop modern methods of diagnostics of acariases, which are the main cause of allergy, allergic dermatoses and other clinical masks of acariases sickness rate growth, we address acarologists of the world to join the research. Our scientific position we are ready to support by full recovery of a group of patients with allergic dermatoses. Why allergic dermatoses? Condition of the skin of this group of patients before and after treatment is visible to anyone. Only the right etiopathogenetic treatment is able to fully free a patient from his disease, and by that to confirm the correctness of the real origin and development of the disease (Zhaxylykova et al., 1994). There is no other method by 100% verifying accuracy of the etiologic theory except for the method of full recovery of a sick person.
Conclusions
To the beginning of XXI century mites play no less part in our life than one thousand years ago. Mites invaded our closest environment, then relocated onto our body, deepened into it and became the cause of no less dangerous diseases than one thousand years ago. At present the development of medical science and equipment allow timely discovering mites on and in the body of each affected in purposeful examination. However the most important meaning for liquidation of acariases have the thorough knowledge of the clinics of the disease, consolidation of efforts of scientists in biological field, practical healthcare workers, and society. The clinical acarology must become one of the leading disciplines of the clinical medicine.
The current situation with acariases among the population requires
1/ Improvement of the methods of finding mites in the skin, mucous tunics, organs and tissues of people. The epidemiological situation in the world requires development of noninvasive methods of diagnostics.
2/ Equipping medical institutions of any structure with appropriate devices for the search of mites in the skin and mucous tunics.
3/ Improvement of the existing methods of finding mites in the organs and tissues of people.
4/ Development and further introduction into the medical practice efficient means for treatment and prevention of acariases in cooperation with reliable pharmaceutical producers.
ACKNOWLEDGEMENTS
We are grateful to the scientists of the world for publications, without which we would not be able to understand in details of the problem of acariases.
Great thanks and obeisance to Academicians Bahiya A. Atchabarov and Michael E. Zeltzer for their support and assistance in the work. We express our gratitude to Academician Turegeldy Sh. Sharmanov and Professor Raisa H. Kadyrova for the opportunity to accomplish works for Ph. D. thesis in the managed by them clinic. Without strong basic scientific school, we would not be able to achieve success in our further work. We are sincerely thankful to Professors Tynyskul S. Teleuova and Vadim G. Uldanov for their participation in our researches. For the great help and participation in the work, we express our gratitude to acarologist Vladimir N. Kusov, Doctor of Biological Science. Obeisance and gratitude to Professor N.N. Ozereczkovskaya (Moscow, Institute of Parasitology named after Martsinovsky) for the objective estimation of submitted in 1982 materials of our invention application. We wish we had more such True Scientists, who pay no attention to which scientific school or clan belong the work’s author, and give objective expert estimation to scientific works!
We are grateful to acarologists Elena V. Dubinina, Cand. Sc. (Biology) (Saint-Petersburg) for the provided opportunity to make a speech on the breakout session under her chairmanship, notwithstanding the secret instructions «not to discuss demodecosis issues» of the chairman of VI All-Union Conference of acarologists in Frunze in 1986. We express gratitude on our own behalf and on behalf of patients to the heads of medical institutions of Almaty (Abdybek T. Turabaev, Mariam K. Kenenbaeva, Amantai B. Birtanov, Zhanar G. Mustafina and others), Kentau (Auesbek M. Malikov) for the opportunity to conduct research works in their institutions. For participation and help in our work we are thankful to all the doctors of these institutions, among them Raisa G. Masheeva, Gulnar M. Dulatova, L.S. Solovyeva, and others.
Special thanks to the chairman of the organizing committee of VI Congress of Acarologists of Europe Mr. Michel Bertrand for the provided opportunity to make a speech in front of acarologists concerning this problem in July 2008.
REFERENCES
Agadzhanjan N. and L.G.Savelyeva. 1997. Ecology of the person, health and the concept of survival. pp.3-19. In: Medical problems of ecology of the person. The collection of proceedings. Ust-Kamenogorsk. Kazakhstan.
Baker A. S. 1999. Mites and Ticks of Domestic Animals. An Identification Guide and Information Source. London. The Stationery Office. 240pp.
Belousova T. A. 2003. Allergodermatoses is illness of the modern civilization. Russian medical magazine. Volume 11. 27: 1538-1542.
Bogdanova E.N. 2005. The acaries harmful for the health of people in city conditions, on the example of Moscow, and system of actions on struggle against them. Medical parasitology and parasitic illnesses. 3: 9-15.
Cunha B.A. 2001. Tick borne Infectious Diseases: Diagnosis and Management. New York, Basel, Marcel Dekker, Inc., 283 pp.
Gerson U., Smiley R.L., Ochoa R. Mites (Acari) for Pest Control. – Oxford, Blackwell Science, 2003. 539 рp.
Gromnatskij N.I. 2005. The handbook of internal illnesses. Moscow. Medical information agency. 812pp.
Jusupova T.J., R.D. Zhaxylykova, A.D. Ahimova, S.T. Sharipova. 1995. Acariases and allergy. Public health of Kazakhstan. 10: 63-65.
Khaitova R.M. 2002. Clinical allergology. A handbook for practical doctors. Moscow. Med.press-inform. 590 pp.
Kiseleva P. 2007. Russia in mites. Izvestiya. 104: 4.
Lobzin J.V, S.S.Kozlov, A.N.Uskov. 2000. The handbook of infectious diseases with the atlas of an infectious pathology. St. Petersburg. 508 pp.
Ponomarev B.A., V.I. Kulagin, G.D. Selisskij, D.K. Novik. 2000. The basic problems of ectoparasitic infections. The bulletin of dermatology. 1: 39 -40.
Roitman V.A. and S.A. Beer. 2008. Parasitism as the form of symbiotic relations. Moscow. Company of scientific publications КМК. 342 pp.
Semenov A.V., A.N.Alexeev, E.V.Dubinina. 2002. Multiple infection by pathogens of acaries - carriers as the risk factor of mix-infection of the person. pp. 30-31. In: Accounting scientific session on results of works 2001. Theses of reports. Zoological institute of the Russian Academy of Sciences. St. Petersburg.
Sergiev V.P. 2006. Production of food as potential biological threat. Medical parasitology and parasitic illnesses. 2: 46-52.
Sokolova T.V. 2001. Itch. New in etiology, epidemiology, clinic, diagnostic, treatment and preventive treatment (lecture). Russian magazine of skin and venereal diseases. 1: 27-39.
Surovenko T.N., L.V. Zheleznova. 2002. Acarological monitoring as made medical strategy by the mite-borne sensibilization. Allergology. 2. Pp. 32-38.
The Sixth European Congress of Acarology. Integrative Acarology. Montpellier 21-25 July 2008. Programme. Abstracts. List of participants. Pp. 89-90.
Vasilevich F.I. and S.V.Larionov. 2001. Demodecosis of animals. Мoscow. Science. 254 pp.
Vasilyeva I.S. 2006. Mites – Inhabitants of Food Stocks Harmful for Human Being’s Health. Medical Parasitology and Parasitic Diseases. 2: 54-58.
Walter David E., H. Proctor. 1999. Mites: Ecology, Evolution and Behaviour. Sydney, University of New South Wales Press and Wallingford, 322pp.
Zhaxylykova R.D. 1979. The beneficial effect of integral camel and mare milk in dietotherapy of sick with chronic hepatites. The auto abstract of the dissertation on competition for scientific degree of the candidate of medical sciences. Frunze. 14 pp.
Zhaxylykova R.D., A.M. Malikov. 1982. The method of diagnostics of demodecosis. The Copyright certificate 1351580.
Zhaxylykova R.D. 1983. About the reason of growth of diseases in XX century. The scab caused by mites or secondary allergy or the Illness by Zhaxylykova. Alma-Ata. 14 pp.
Zhaxylykova R.D. 1990. Demodex Mites and their biological value. (Data from the literature, hypotheses and facts). The deposited works. №4213-В90.
Zhaxylykova R.D., M.K. Kenenbaeva. 1990. To the question of diagnostics of demodecosis. The bulletin of the Academy of Sciences of Kazakh SSR. 4: 69-71.
Zhaxylykova R.D. 1991. The Demodecosis is the mite-born disease. The health. 3: 6-7.
Zhaxylykova R.D. 1992a. Diagnostics of acariases and their complications. The State Committee of Republic of Kazakhstan on economy. The Information leaflet. Almaty. 4 pp.
Zhaxylykova R.D. 1992b. The Demodecosis and associative illnesses. The bulletin of the Academy of Sciences of the Republic of Kazakhstan. 4: 84-88.
Zhaxylykova R.D., A.M. Malikov. 1994. Diagnostics of allergic, skin and other variants of associative mite-born illnesses. News of sciences of Kazakhstan. 1: 59-60.
Zhaxylykova R.D., T.U. Usupova, G.M. Pichhadze. 1994. The method of medical treatment of patients with pollinoses and allergic all-year-round rhinites. The preliminary patent.
Zhaxylykova R.D. 1999. An allergy as the reason of growth of diseases to the beginning of the third millenium. (Allergy = Acarias). Almaty. Akil kitabi. 192 pp.
Zhaxylykova R.D 2000. The allergy is a clinical mask of acariases. Medicine. The international professional magazine. 1: 19-22.
Zhaxylykova R.D. and D.A. Zhunusova. 2001. Allergy is a not diagnosed acariasis. The bulletin of the Ministry of Education and Science of the National Academy of Sciences of the Republic of Kazakhstan. 4: 84-89.
Zhaxylykova R.D., V.N. Kusov. 2001. The acary Gamazoidea - agents of dermatoses. Medicine. The international professional magazine. 1: 33-34.
Zhaxylykova R.D. 2002a. Akariasis and collagenoses. News of the Ministry of Education and Science of the Republic of Kazakhstan, National Academy of Sciences of the Republic of Kazakhstan. Biological series. 6: 16-32.
Zhaxylykova R.D. 2002b. Everyone has Acariasis but it is possible and necessary to cope with it. Science and the higher school of Kazakhstan. 24(46): 5.
Zhaxylykova R.D., A.Sh. Seisenbaev. 2002. Acaries and rheumatic illnesses. Medicine. The international professional magazine. 5: 17-20.
Zhaxylykova R.D. 2006a. The allergy is acariasis. Bulletin of healthy way of life. 19: 13.
ZhaxylykovaR.D. 2006b. The true diagnosis is not a verdict, but panacea! The capital prospectus. 50 (327): 6.
Zhaxylykova R.D. 2006c. “The truth about Allergy”. Business-region of Kazakhstan. 1 (65): 14.
Zhaxylykova R.D. 2007a. Acariasis is the key problem of the clinical medicine. (Message I).Valeology. 1: 7-9.
Zhaxylykova R.D 2007b. Acariasis is the key problem of clinical medicine. (Message II). Valeology. The scientific and practical journal. 2: 6-8.
Zhaxylykova R.D. 2007c. Acariasis is the key problem of the clinical medicine. (Message III).Valeology. Health – Illness – Recovery. The scientific and practical journal. 3: 13-15.
Zhaxylykova R.D. 2007d. Harmful action of Acari on human being (Literature Review. Part I). Astana Medical Journal. № 1 (37): 8-10.
Zhaxylykova R.D. 2007e. Harmful action of Acari on human being (Literature Review. Part II.). Astana Medical Journal. 6 (42): 23-27.
Zhaxylykova R.D. 2007f. Harmful action of Acari on human being. (Literature Review. Part III). Astana Medical Journal. 9 (45): 30-34.
Zhaxylykova R.D., Zh.E. Musin, M.H. Bajmuhanov, M.A. Raeva, E.A. Mahambetova. 2008. How to get rid of an allergy. Astana. State Publishing House. 132 pp.